
NASAL AERODYNAMICS and RHINOSINUSITISES
PRIMARY VALVE OF THE NOSE - IT'S HIS CAVERNOUS BODIES
Relationship between two parallel respiratory structures in the nose
The main cause of the night snoring is violations of the nasal aerodynamics
The functionality of the small ostiums of the nasal sinuses
Critical comparison of opposite opinions about the function of the nasal sinuses using Occam's Razor
The real significance of the limen nasi
VARIANTS OF NASAL AERODYNAMICS
NORMOGRAM OF NASAL AERODYNAMICS
PHYSIOLOGICAL BRIDGE REPRESENTED BY THE NASAL VALUE
SURGICAL RECONSTRUCTION OF NASAL AERODYNAMICS
SEPTOPLASRY UNDER CONTROL OF NASAL AERODYNAMICS
CONTRAINDICATION TO SEPTOPLASTY
PROTECTION OF THE INFERIOR NASAL PASSAGE FROM INSPIRATION
THE INSIDIOUSNESS OF THE UNILATERAL "SOUTHERN" NASAL AERODYNAMICS.
SNORING WHEN NASAL RESPIRATION IS SAVED.

inferior turbinate is largeness.
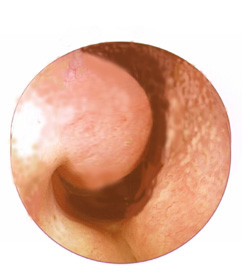
Fig. 2 Southern type of nasal aerodynamics
inferior turbinate is small-sized.
 |
Surgical reconstruction of nasal aerodynamics(Uliyanov Y.P. Surgical reconstruction of nasal aerodynamics. XVI World Congress of Otolaryng. Head and Neck Surg. Sydney, Australia, 2-7 March, 1997: 1591-1595). |
||||
SUMMARYTwo main variants of the nose anatomy – «northern» and «southern» have been established. Having proved these data in over 1000 patients with a high rate of seasonal rhinopharyngitis, we have de-veloped a new method of plastic repair which we have performed in 100 patients. The method provides for construction of the air-directing «steering mechanism» in those with the «southern» type nose, to create a kind of physiologic bridge.INTRODUCTIONOur studies of separate air flows in the nasal passage ways at in-halation and exhalation [1] have shown that earlier authors were right each in his way, as we have in fact detected two extreme variants of nasal aerodynamics which we have tentatively named the northern and southern type noses. We have chosen to call the northern type nose the normal one as possessing the best construction in what concerns its protective proper-ties (Fig.1). This type features the following: as inhalation, the main airstream is drawn in through the median nasal passage, reaching 80 arbitrary units (AU), with ten AU coming in through the upper pas-sage and 20 AU through the lower one, whereas the distribution of air at exhalation in the lower and median nasal passages amounts to 80 and 20 AU, respectively. The southern type nose is apt only for warm humid climate zones, featuring the reverse distribution of air flows (Fig.2). At inhala-tion, the main airstream is drawn in through the lower nasal passage, reaching 80 AU, with ten AU coming in through the upper passage and 20 AU through the median one, whereas the distribution of air at exha-lation in the median, lower and upper nasal passages amounts to 80, 20 and 10 AU, respectively.PATIENTS AND METHODSAn examination of 1000 patients, aged from two to 86 years, who regularly suffer from common colds, has shown that all of them feature defective aerodynamics of the nose as opposed to the norm, having mainly the southern type nose. The normal graph of nasal aerodynamics was re-corded in only 22% of 300 obviously healthy people who suffered from common colds less than once in the period of four to five years. A comparative analysis of the features of the anatomical structure of the nasal passages in these two extreme groups of people has shown that the southern type nose is characterized by the lower and median nasal passages being united in a kind of the common passage with wide lumen between the nasal septum and lateral nasal wall. The inferior turbinate bone is small and somewhat atrophic (Fig.2-1). The northern type nose features strict boundaries between the median and lower nasal passages. The inferior turbinate bone is of a medium or large size (Fig.4-1). This bone nearly comes in contact with the nasal septum, which provides for the demarcation between the nasal passages. Therefore, the developed inferior turbinate bone shifts the main airstream at inhalation to the median nasal passage. The absence of the bone is known to return this stream to the lower passage. The above statements suggest that the well-developed inferior turbi-nate bone is necessary for formation of this physiologic bridge demarcating the lower and median nasal passages to direct the main airstream at inha-lation into the median nasal passage. Therefore, formation of this physiol-ogic bridge by increasing the inferior turbinate bone will transform aerody-namics of the southern type into its northern counterpart. The constructive solution of this problem has turned out to be paradoxical in respect to the common opinion of the necessity to dissect the synechiae in the nose between the inferior turbinate bone and nasal septum. Now we understand quite clearly that it is these adhesions be-tween the inferior turbinate bone and the nasal septum that are situated at the area of the physiological bridge, in fact playing the role of the air-directing "steering gear" which provides for a cardinal transformation of aerodynamics of the nose and its protective properties. This is why we have decided to make this air-directing "steering gear" in the area of the physiologic bridge with double blood supply from two sides, which would strengthen it to the maximum possible de-gree and bring about the greatest effect (Fig.3). Surgery was indicated in patients with impaired aerodynamics of the nose (the southern type nose) with chronic rhinopharyngitis with a severe course and manifest atrophic and subatrophic mucosa. Under local anesthesia, a soft-tissue flap is formed from the mu-cosa of the nasal septum (Fig.4-B) with there incisions: in the lower edge of the nasal septum along the nasal floor at a length of 1.3 to 3 cm; then, from the anterior and posterior edges of this incision two vertical incisions are made at a height of 2.0 cm (Fig.4: 1,2). The incised flap is then separated from the lower edge until the end of the vertical inci-sions. As a result, a movable soft-tissue pedicle flap is formed which is lifted upwards (Fig.4: 8). A similar soft-tissue flap, also under local an-esthesia, is formed from the mucosa of the facing area of the exterior nasal wall (Fig.4-A), but in a mirror-like reverse fashion: the anterior and posterior vertical incisions are performed (Fig.5: 4-5) from the pedicle of the flap of the nasal septum upwards to 2.0 cm where they are united by a longitudinal incision parallel to the floor of the nasal cavity (Fig.5: 6). This flap is then separated from the superior edge down to the inferior edge of the vertical incisions. This results in formation of a soft-tissue flap with a pedicle below. This flap is upwards (Fig.5: 7). To fix this flap in the horizontal position, a soft rubber tube is placed there-under (Fig.5: 9). Then the bare side onto its counterpart of the lower flap. As a result, both flaps stick immediately. In this way, a new air-directing passage is formed to restore the protective function of the nose. The last stage of surgery is a soft packing of the wound in the nose with pressing of the upper flap to the lower one. In the postoperative period, antibacterial and anti-inflammatory therapy is carried out during seven to ten days. The pack from the nose is removed at day five to seven, when the pack no longer sticks to the part of the bare surface of the exterior nasal wall. At day 10 or 12, as the flap is fastened, the rubber tube placed underneath is removed. Full healing takes from two to three weeks. In a month, the tis-sues of the nose injured during surgery regain normal aspect completely, and become pale and firm. They retain this state for many years in fu-ture. There were no complications.RESULTS:This new air-directing passage makes the airstream divide into two separate ones: the superior and the inferior, which go opposite ways, considerably differing from the original preoperative stream. If this flap is placed correctly, the main airstream is directed upwards into the median nasal passage at inhalation 80 AU, with 10 AU going into the lower nasal passage, which corresponds to the normal graph of nasal aerodynamics. As a result, the condition of the nasal mucosa consid-erably improves in first weeks and months after surgery. The otherwise dry and subatrophic mucous membrane of the nose becomes soft and moist without any signs of inflammation, The atrophic mucosa also is altered to the better, as it gets moist and more viable. The method was applied to treat 100 patients aged from four to 65 years. There were 64 females and 36 males. The predominant age group consisted of persons in the age range from 20 to 35. During the first twelve months after surgery, the results were good in all cases. One year after surgery, the flap broke in two young women (aged 17 and 22) because of intensive blowing the nose in acute common cold. Follow-up of over 30 patients during over ten years has shown that the results were lasting and good.REFERENCES:1. Cole P. Some aspects of temperature, moisture and heat relation-ships in the upper respiratory tract. J.Laryngol.Otol., 1953, 449-4562. Ingelstedt S. Study on the conditioning of air in the respiratory tract. Acta Otolaryngol., 1956; 131: Suppl.1-10. 3. Ulyanov Y.P. Nose aerodynamics. Arch Otolaryngol. Head Neck Surg. 1995; 121: 352. 4. Ulyanov Y.P., Polivanov P.P. Russian patents ąą1,572,505, 1,602,472. 5. Ulyanov Y.P. Method of reconstruction of the protective function of the nose. Russian patent ą95105086. Legends for Illustrations:Fig. 1: Distortion of the nasal septum forming the "northern" type of the nasal aerodynamics at the right.Fig. 2: Construction of the "northern" type of the nasal aerodynamics also at the left, with the distortion of the nasal septum to the right. Fig. 3: Distortion of the nasal septum because of the spine at the right. Fig. 4: Construction of a new air-directing "steering gear" at the left, with the "northern" type of the nasal aerodynamics at the right. Fig. 5: Distortion of the nasal septum in the compensatory variant. 1) The nasal septum.
|
|||||

Fig. 1
|

Fig. 2
|

Fig. 3
|
|||

Fig. 4.
|

Fig. 5.
|
||||
| A. Exterior nasal
B. Nasal septum. C. Nasal floor. |
1.
Anterior incision.
2. Posterior incision. 3. Inferior incision. 4. Anterior incision. |
5. Posterior
incision.
6. Superior incision. 7. External flap. 8. Internal flap. 9. Rubber tube.wall.
|
|||

